April is National Autism Awareness month in the United States. Early recognition improves outcome. This April we will post a series on the recognition of autism in a baby and in a toddler, as well as a personal story. — Drs. Kardos and Lai
Home videos of children diagnosed with autism reveal that even before their first birthdays, many autistic children demonstrate abnormal social development that went unrecognized.
Autism is a communication disorder where children have difficulty relating to other people. Continue Reading
The school nurse calls to say, “I have your child here with me and she has a sore throat. I think you should take her to the doctor to see if it’s strep throat.”
What IS strep throat?
Strep throat is a throat infection caused by Group A streptococcus (Strep pyogenes) bacteria. Symptoms can include sore throat, Continue Reading
Does your kid spit out medicine? Clamp her jaws shut at the sight of the antibiotic bottle? Refuse to take pain medicine when she clearly has a bad headache or sore throat?
Sometimes medicine is optional but sometimes it’s not. Here are some ways to help the medicine go down:
Don’t make a fuss. We mean PARENTS: don’t make a fuss. Stay calm. Explain that you are giving your child medicine “for your sore throat,” for example. Calmly give her the pill to swallow or the medicine cup or syringe filled and have her suck it down, then offer water to drink. If you make a BIG DEAL or warn about the taste or try to hurry your child along, she may become suspicious, stubborn, or flustered herself. Calmness begets calm.
What if she hates the taste?
Most medication can be given with a little chocolate syrup or applesauce (yes, Mary Poppins had the right idea). Check with your child’s pharmacist if your child’s particular prescription can be given this way.
Often, your pharmacist can add flavor to your child’s prescription.
Check if your child’s medicine comes in pill form so she doesn’t have to taste it at all.
Try “chasing” the medicine down with chocolate milk instead of water to wash away a bad taste quicker.
Use a syringe (no needle of course) to slowly put tiny bits of liquid medicine in the pocket between her outer teeth and her cheek. Sooner or later she will swallow. After all, she swallows her own saliva. ( A factoid: an adult swallows up to 1.5 liters of saliva a day.)
DO NOT mix the medication into a full bottle or a full cup and expect that your child will finish it all. There is a good chance that the child will not finish the bottle and therefore not finish the medication. If mixing into a liquid, better to suck up the medicine into a measuring syringe and then, if needed, suck up an addition little bit of juice or Gatorade to attempt to hide the flavor and get the full dose in at once.
WHAT IF SHE THROWS UP THE MEDICATION? Call your child’s doctor. If the medication was not in the stomach for more than 15 minutes, we will often not count it as a dose and may instruct you give another dose.
WHAT IF SHE CAN’T SWALLOW PILLS? If your child can swallow food, she can swallow a pill. Dense liquids such as milk or orange juice carry pills down the food pipe more smoothly than water. Start with swallowing a grain of rice, a cake sprinkle, or a tic-tac. For many kids, it is hard to shake the sequence of biting then swallowing. Face it. You spent a lot of time when she was toddler hovering over her as she stuffed Cheerios in her mouth, muttering “bite-chew-chew-swallow.” Now that you want her to swallow in one gulp, she is balking. Luckily, most medication in pills, although bitter tasting, will still work if you tell your child to take one quick bite and then swallow. The exception is a capsule. The gnashing of little teeth will deactivate the microbeads in a capsule release system. If you are not sure, ask your pharmacist.
WHAT IF ALL ATTEMPTS AT ORAL MEDICINE FAIL? Talk to your child’s doctor. Some liquid antibiotics come in shot form and your pediatrician can inject the medicine (such as penicillin), and some come in suppository form; Tylenol (generic name acetaminophen) is an example. You can buy rectal Tylenol if sore throat pain or mouth sores prevent swallowing or if your child simply is stubborn. Sometimes you just have to have one adult hold the child and another to pry open her mouth, insert medicine, then close her mouth again.
HAVE AN EAR DROP HATER? First walk around with the bottle in your pocket to warm the drops up. Cold drops in an ear are very annoying. (In fact, if cold liquid is poured into the ear a reflex occurs that causes the eyes beat rapidly back and forth). Use distraction. Turn on a movie or age-appropriate TV show, have your child lie down on the couch on her side with the affected ear facing up. Pull the outside of her ear up and outward to make the ear opening more accessible, then insert the drops and let her stay lying down watching her show for about 10 minutes. If you need to treat both ears, have her flip to the other side of the couch and repeat. Another option: treat your child while she sleeps.
AFRAID OF EYE DROPS? If your child is like Dr. Kardos who is STILL eye-drop phobic as a grown-up, try one of two ways to instill eye drops. Have your child lie down, have one person distract and cause your child to look to one side, insert the drop into the side of the eye that your child is looking AWAY from. She will blink and distribute the medicine throughout the eye. Alternatively, have your child close her eyes and turn her head slightly TOWARD the eye you need to treat. Instill 2 drops, rather than one, into the corner of her eye nearest her nose. Then have her open her eyes and turn her head slowly back to midline: the drops should drop right into her eye. Repeat for the second eye if needed.
HATE CREAM? Some kids need medicated cream applied to various skin conditions. And some kids hate the feeling of goop on their skin. These are often the same kids who hate sunscreen. Again, distraction can help. Take a hairbrush and “brush” the opposite arm or some other area of the body far away from the area that needs the cream. Alternatively, apply the cream during sleep. Another option- let your child apply his own cream- this gives back a feeling of control which can lead to better compliance with medicine. It also will help him to feel better faster. IF your child is complaining about stinging, try an ointment instead. Ointments tend to sting less than creams.
Of course, as last resort, you can always explain to your child in a logical, systematic fashion the mechanism of action of the medication and the future implications on your child’s health outcome.
If you choose this last method, you should probably have some Hershey’s syrup nearby. Just in case.
It’s time for another Two Peds in a Pod photo quiz.
The question: What’s depicted in this photo?
If you answered: a pen, a thumb nail drive, or an asthma inhaler, you would be wrong.
Kids use these devices, which purposely look like common innocuous objects, to inhale electronic cigarettes (e-cigarettes). Vaping, also called “Juuling” and an even more concentrated form of vaping, called “dripping,” is unfortunately popular among teens. It’s unhealthy: the stuff that the kids are inhaling contains nicotine and other chemicals.
Ask your middle schooler or high schooler. They most likely have seen these devices if they have not actually used one.
Parents need to know kids are vaping in school as well as outside of school. Unlike conventional cigarettes, it’s easy for the kids to hide: no smoky smell, no cigarette cartons. The vaping liquid or “e-juice” comes in all kinds of “kid friendly” flavors such as gummy bear, fruit, or chocolate, and the devices needed to inhale them look like items in every kid’s pencil case or backpack.
It’s easy for kids to get the e-juice on the internet because online stores don’t always ask for proof of age (legal age to buy is 18 years in the US). Most e-juices contain nicotine, which is addictive. Emerging data show that kids who vape are more likely to go on to use regular cigarettes than kids who do not vape.
Bottom line: Vaping, or using electronic cigarettes, is unhealthy and addictive, and startlingly easy for kids to hide.
Nope, warthogs don’t actually have warts. But kids often do!
Emma’s dad and I both peered at the filamentous growth dangling from his nine year old’s right nostril. “Yes,” I said, “it’s definitely a wart.”
Emma’s dad offered, “When I was a kid, I heard the way to get rid of a wart was to cut a potato in half, rub it on the wart, and bury the potato in the backyard. Legend had it, by the time the potato disintegrates, the wart will be gone.”
“I wish it were so easy,” I replied.
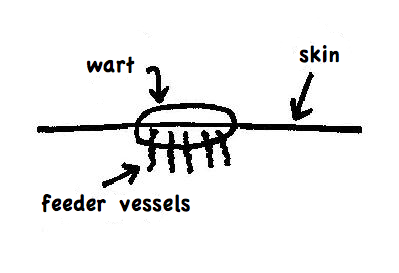
Warts are caused by skin-dwelling viruses. On the feet, warts can sometimes be mistaken for calluses. One distinguishing feature is that warts sit in the skin like this:
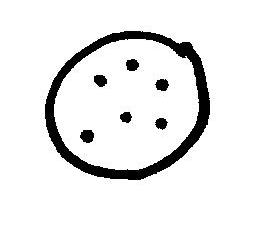
Fine “feeder” blood vessels extend from the wart into the skin. Therefore, if you scrape off the top layer of a wart, a dotted pattern usually appears from above. The dots will not appear in a callus. View from above:
There are simply no glamorous ways to get rid of warts. Most treatment modalities destroy warts by pulverizing the home they live in, a.k.a. your skin. Your doctor may be armed with various agents such as liquid nitrogen or dimethyl ether propane, which produces a chemical “freeze” and dries up the wart. Another agent called cantharidin (otherwise known as “beetle juice”) is a caustic liquid derived from the blister beetle. Application of beetle juice causes the warts to blister.
Some doctors will even manually take a scalpel and cut out the warts.
Like I said, there are no glamorous treatments. However, more gentle creams which stimulate the immune system, such as Imiquimod (Aldara) show some promise in children. Other compounds such as 5-fluorouracil can be topically applied or injected and treatments such as pulsed dye laser therapy have mixed reviews.
Over-the-counter remedies exist in a milder form. Commonly used wart removers such as Compound W, Dr Scholl’s Clear Away Wart, and Duofilm all contain salicylic acid. The acid slowly dries up the warts. When applying salicylic acid, after a few applications make sure you peel the dead crusty top layer off the wart. Without peeling, future medicine will not reach the wart. These methods can take weeks to months to work, but they do work.
And don’t forget the duct tape. Duct tape, the great all-purpose household item, has also been shown to speed up the resolution of warts. Scientists hypothesize the constant presence of the adhesive somehow stimulates a natural immune response. If you try duct tape, have your child wear the duct tape over the wart for several days in a row and then give a day off. If the wart is on a hand or foot, the tape tends to fall off during the day: just re-apply some tape at bedtime. Effects should be seen within a couple of months if not sooner. Now, the original study that showed duct tape was helpful, was followed by a study which showed duct tape was not helpful. Some hypothesize that the results differ because silver sticky duct tape was used in the initial study, while the later study used less sticky duct tape. So be sure to use the old-fashioned silver duct tape.
The prevention of warts is tricky. Some people just seem genetically predisposed. However, your best bet for keeping warts away is to keep your child’s skin as healthy as possible. Warts tend to gravitate towards areas of skin broken down by friction such as feet or fingers. Liberally apply moisturizing creams daily to prone areas. After a summer of wearing flip-flops and walking on the rough cement by the side of a swimming pool in bare feet, many children end up with warts on the bottom of their feet. I know a teen whose warts on the tips of her fingers stemmed from months of guitar strumming.
Turns out that even without treatment, 60% percent or more of all warts will disappear spontaneously within two years.
Coincidentally, I think that’s also the time it takes for a potato half to disintegrate.
When the Tin Man was a child in Oz, I’m sure his pediatrician never told his parents, “Has anyone ever said your child has a heart murmur? I hear one today.”
I know that when I tell parents about a heart murmur in their child, their hearts skip and jump. But not all heart murmurs are bad.
What is a heart murmur?
A heart murmur is an extra sound that we pediatricians hear when we listen to a child’s heart with a stethoscope. A normal heart beat sounds like this: “lub, dub. lub, dub. lub, dub.” A heart murmur adds a whooshing sound. So what we hear instead is “lub, whoosh, dub” or “lub, dub, whoosh.”
The “whoosh” is usually caused by blood flowing through a relatively narrow opening somewhere in or around the heart. Think of your blood vessels and heart like a garden hose. If you run the water (blood) very hard, or put a kink or cut a hole in the hose, the whoosh of the water grows louder in those locations.
Heart murmurs signal different issues at different ages.
In a newborn, some types of heart murmurs are expected. Normal newborn hearts contain extra holes that close up after the first hours or days of birth. One type of murmur occurs as the infant draws in his first breath and holes in the heart, present inside the womb, begin to seal. As the holes get narrower, we sometimes hear the “whoosh” of blood as it flows through the narrowing opening. Then these holes close completely and the murmur goes away.
However, some murmurs in infancy signal “extra holes” in the heart. As pediatricians, we experience our own heart palpitations when moms want to leave the hospital early with their infants who are less than 48 hours old. We worry because many infants who have abnormal hearts may not develop their abnormal heart murmurs and other signs of heart failure until the day or two after birth.
Preschool and early school-age children often develop “innocent” heart murmurs. “Innocent” implies that extra blood flows through their hearts, but the hearts are structurally normal. These murmurs are fairly common and can run in families. However, there are some significant heart problems which do not surface until this age. For this reason, remember to schedule those yearly well child checkups.
For teens, during the pre-participation sports physical, pediatricians listen carefully for a murmur that may indicate that an over grown heart muscle has developed.
What else can cause a heart murmur?
Holes are not the only culprit behind a murmur. The whoosh sound can also arise when a person is anemic and blood flows faster than normal. In anemic kids, the blood flows faster because it lacks enough oxygen-carrying red blood cells and the heart needs to move blood faster in order to supply oxygen to the body. The most common cause for anemia is a lack of eating enough iron-containing foods. Subsequently, we hear these flow murmurs in children whose diets lack iron, in teenagers who grow rapidly and quickly use up their iron stores, and in girls who bleed too much at each period. Replenishing the iron level makes a heart murmur from anemia go away.
Even a simple fever can cause a heart murmur on physical exam. The murmur goes away when the fever goes away.
Pediatric health care providers can often distinguish between “innocent” heart murmurs and not-so- innocent heart murmurs by the sound of the murmur itself (not all “whooshes” sound alike). If any question exists, your child will be referred for more testing, which could include a chest x-ray, an EKG (electrocardiogram), an ECHO (echocardiogram, or ultrasound of the heart), or evaluation by a pediatric cardiologist.
If your child’s pediatrician tells you that your child has a heart murmur, “take heart.”
Many times a murmur comes and goes or just becomes part of your child’s baseline physical exam. Even if your child has a serious heart problem, most cases respond well to medication, surgery, or both. While not all heart problems cause heart murmurs, and while not all murmurs signal heart problems, the presence of a heart murmur in a child can signal that your child needs further testing.
Unless, of course, your child is the Tin Man. In this case, extra sounds indicate that your child needs more oil!
The recent Parkland shooting in Florida is causing many to wonder how to support the emotional health of boys in their families and communities. We welcome therapist Dina Ricciardo’s words of wisdom— Drs. Kardos and Lai
Your son is crying. A mad dash across the playground has led to a spectacular trip and fall, complete with a bloody knee and hands full of dirt. Part of you wants to hold him on your lap and console him until he stops crying. The other part of you wants to firmly wipe away his tears and tell him to be brave. Which part of you is right?
In a world where there is a great deal of emphasis placed on the emotional health of girls, our boys are frequently overlooked. While girls are typically encouraged to develop and express a broad range of emotions, boys are socialized from a young age to suppress their feelings. As a result, many boys and men struggle to express fear or sadness and are unable to ask for help. It is time for us adults to stop perpetuating stereotypes and myths about manhood, and help each other raise emotionally healthy boys. Here are five ways for us to do so:
Make his living environment a safe space to express emotions. Give your son permission to express all of his feelings. Boys typically do not have the freedom to show the full range of their emotions in school and out in the world, so it is essential that they have that freedom at home. Nothing should be off limits, as long as feelings are expressed in a manner that is not destructive.
Expose him to positive male role models. Boys need to be exposed to positive male figures who can to indoctrinate them into their culture and teach them how to be men. It is an important rite of passage in a boy’s development. Take a look around your social ecosystem and ask yourself, “Who would be good for my son?” Other parents, coaches, teachers, and pastors are examples of individuals who can play a positive role in his life.
Understand your unique role. Each parent plays a unique role in the development of a son, and that role changes over time. A mother is a son’s first teacher about love and what it looks like, and this dynamic can breed a particular kind of closeness. As a boy grows and begins to develop his sexuality, however, it is natural for him to pull away a bit from his mother and turn more towards his father for guidance. While this distance can be unsettling for mom, it marks a new phase in a son’s relationship with his father, who typically provides a sense of security and authority in a family as well as support for a boy’s developing identity. Mothers still play an important role, but that role may look different. As parents, it is important to re-evaluate what our sons need from us at each stage of their development.
Look at the world with a critical eye. Our culture not only glorifies violence, it equates vulnerability in males with weakness and attempts to crush it. That does not mean we have to accept this paradigm. Talk honestly with your son about how and when to be gentle and compassionate, educate him on how the world view softness in men, and never tolerate anyone shaming him when he exhibits these traits. There is no shame in showing vulnerability, it is actually an act of courage.
Take a look in the mirror. Whether you are a mother or a father (or both), be honest with yourself: what are your beliefs about manhood? Do you feel safe expressing all of your feelings, or are some of them off-limits? If you are perpetuating negative stereotypes about men or are not comfortable with a full range of emotions, then your son will follow in your footsteps. Regardless of our own gender, we cannot expect our children to be comfortable with their feelings if we are not comfortable with our own.
There are times when insuring the emotional health of your son will feel like an uphill battle. Keep the conversation open, and do not be afraid to talk with others about the dilemmas of boyhood and manhood. And if you are looking for an answer to the playground dilemma, then I will tell you that both parts of you are right. Sometimes our sons need loving compassion, and sometimes they need a firm nudge over the hump. You know your child better than anyone else, so it is up to you to decide which approach to use and when.
Dina Ricciardi is a psychotherapist in private practice treating children, adolescents, and adults in Doylestown, PA. She specializes in disordered eating and pediatric and adult anxiety, and is also trained in Sandtray Therapy. Ricciardi is a Licensed Social Worker and a member of the Academy of Certified Social Workers. She can be reached at [email protected].
We welcome Bereavement Counselor Amy Keiper-Shaw who shares with us how to discuss the death of a pet with your child. –Drs. Lai and Kardos
When I first graduated from college I worked as a nanny. One day the mom shared with me that their family goldfish recently died. As this was her daughter’s first experience with death, we schemed for nearly 20 minutes to find the best way to talk to her child. The mom and I thought it could be an excellent teaching moment.
Even when it isn’t flu season, we pediatricians wash our hands about sixty times a day, maybe more. This frequent washing, in combination with cold winter air, leads to dry, chapped hands. Here are the hands of a patient. Do your children’s hands look like these?
To prevent dry, chapped hands:
• Don’t stop washing your hands, but do use a moisturizer afterwards. Also use warm but not hot water. Hot water removes protective oils from skin.
• According to the American Academy of Dermatology, hand sanitizer can prevent the drying that accompanies frequent hand washing. However, we can tell you from experience that once your hands are already chapped and cracked, the alcohol content in the sanitizers stings sensitive skin. So if your child’s hands are already chapped, stick with water and soap.
• Wear gloves or mittens as much as possible outside even if the temperature is above freezing. Remember chemistry class—cold air holds less moisture than warm air and therefore is unkind to skin. Gloves will prevent some moisture loss. Having difficulty convincing your child to wear gloves? Point out that refrigerators are kept around 40 degrees Fahrenheit or below. Tell your kids that if they wouldn’t sit inside a refrigerator without layers, then it would be wise to wear gloves.
• Before exposure to any possible irritants such as the chlorine in a swimming pool, protect the hands by layering heavy lotion (e.g. Eucerin cream) or petroleum based product (e.g. Vaseline or Aquaphor) over the skin.
To rescue dry, chapped hands:
• Prior to bedtime, smother hands in 1% hydrocortisone ointment. Avoid the cream formulation. Creams tend to sting if there are any open cracks. Take old socks, cut out thumb holes and have your child sleep at night with the sock on his hands. Repeat nightly for up to a week. Alternatively, for mildly chapped hands, use a petroleum oil based product such as Vaseline or Aquaphor in place of the hydrocortisone.
• If your child has underlying eczema, prevent your child from scratching his hands. An antihistamine taken orally such as diphenhydramine (Benadryl) or cetirizine (Zyrtec) will take the edge off the itch. Keep his nails trimmed to avoid further damage from scratching.
• For extremely raw hands, your child’s doctor may prescribe a stronger cream and if there are signs of a bacterial skin infection, your child’s doctor may prescribe an antibiotic.
Happy moisturizing. Remember smearing glue on your hands and then peeling off the dried glue? It’s not so fun when your skin really is peeling.
In light of the recent school shooting in Parkland, Florida, you may be left wondering if, and how, to explain this or other tragedies to your children.
Understand that kids sense your emotions even if you don’t tell them. Not telling them about an event may make them concerned that they are the cause for your worried hushed conversations. Break away from your discussion with adults to say, “ Do you know what we are talking about? We are not talking about you.”
Even though an event may be far away, media makes it seem as if it happened next door, and sooner or later your children will see or hear about it. Tell the facts in a straight forward, age appropriate manner. Answer questions and don’t be afraid to answer with an “I don’t know.” Preschoolers are concrete in their thinking—dragons are real and live under their bed, so don’t put any there that do not exist. For a preschooler a simple “Mom is sad because a lot of people got hurt,” will suffice. Young school age kids will want to know more details. And be prepared to grapple with more high level questions from teens.
Look for the helpers. Mr. Rogers who hosted Mister Roger’s Neighborhood for 30 years, tells this story about seeing scary things on the news: “My mother would say to me, ‘Look for the helpers. You will always find people who are helping.’ To this day, especially in times of ‘disaster,’ I remember my mother’s words, and I am always comforted by realizing that there are still so many helpers-so many caring people in this world.”
What if the kids ask, “Will that happen here?” or “Why did that happen?” Again, reassure in a simple straight forward manner. For instance you can say, “Many people are working hard to prevent something like that here.” Consider answering the question with a question. Asking “What do you think?” will give you an idea of exactly what your child fears. You can also reach out to other family supports for help with answers. Say to your child, ”I wonder what our minister or school counselor has to say about this, let’s ask.”
Routine is reassuring to children, so turn off the background 24 hour television and internet coverage and make dinner, take them to sports activities, and get the homework done.
Give your kids something tangible to do to be helpful. Help them set up a coin donation jar at school or put aside part of their allowance for a donation.
If your child seems overly anxious and fearful, and her worries are interfering with her ability to conduct her daily activities, such as performing at school, sleeping, eating, and maintaining strong relationships with family and friends, then seek professional help.
• Young children are curious. They are often unable to remember or follow safety rules. Teens are impulsive, and naturally tend to be moody. When combined with access to firearms, the consequences can be tragic and permanent.
• The safest home for children and teens is one without guns. If you do have a gun, you can greatly reduce the risk of a child being injured or killed by storing the gun unloaded and locked, with the ammunition locked in a separate place.
Parent your children so they feel secure in themselves and secure in the world around them. You may not hold the answers to why a tragedy strikes, but you do hold the ability to comfort and reassure your children.





 Does your kid spit out medicine? Clamp her jaws shut at the sight of the antibiotic bottle? Refuse to take pain medicine when she clearly has a bad headache or sore throat?
Does your kid spit out medicine? Clamp her jaws shut at the sight of the antibiotic bottle? Refuse to take pain medicine when she clearly has a bad headache or sore throat? It’s time for another Two Peds in a Pod photo quiz.
It’s time for another Two Peds in a Pod photo quiz.




 In light of the recent school shooting in Parkland, Florida, you may be left wondering if, and how, to explain this or other tragedies to your children.
In light of the recent school shooting in Parkland, Florida, you may be left wondering if, and how, to explain this or other tragedies to your children.