Chatting with Janet Zappala: Food for Thought Episode-help for overweight kids and picky eaters
In case you missed the live internet radio show- hit the arrow to tune in here:
In case you missed the live internet radio show- hit the arrow to tune in here:

 Pertussis is “whooping cough,” also known as the “100 day cough.” In children and adults, the disease starts out looking like a garden-variety cold, complete with runny nose, runny eyes, and mild cough. Sometimes fever is present, sometimes not. However, after a few days, coughing spasms emerge – severe, persistent coughing spasms that go on and on and on. In between coughing fits, children may appear okay.
Pertussis is “whooping cough,” also known as the “100 day cough.” In children and adults, the disease starts out looking like a garden-variety cold, complete with runny nose, runny eyes, and mild cough. Sometimes fever is present, sometimes not. However, after a few days, coughing spasms emerge – severe, persistent coughing spasms that go on and on and on. In between coughing fits, children may appear okay.
There is no treatment except to “ride it out” and the cough can last up to three months. Doctors prescribe antibiotics to a child with pertussis because antibiotics can decrease how much a person with whooping cough will spread it to others. Close contacts of kids with pertussis may also receive antibiotics to reduce their chance of getting pertussis.
Whooping cough gets its name from the “whoop” noise kids make after a coughing fit. The fits leave them so breathless that it’s difficult to take a breath in again after the coughing spell. To hear the “whoop” with coughing fit, visit www.whoopingcough.net.
Teens and adults with whooping cough don’t tend to make the whoop sound because their airways are bigger, but the coughing spasms can leave them feeling like they might throw up or pass out. Some in fact do end a coughing fit with vomiting or fainting.
Babies don’t make the whoop either. Instead, babies with pertussis simply cannot catch their breath and stop breathing. That is why babies are the ones who tend to die from this illness. Dr. Lai and I both have watched over hospitalized infants blue from pertussis.
Thankfully, we have a vaccine that is effective at preventing pertussis. The “P” in pertussis is the “P” in the DtaP vaccine that children receive as babies, usually at two, four, and six months of age. The DtaP vaccine is then next given after the first birthday, another between ages four and six years old, and another at age eleven years. Teens who have not received the pertussis vaccine since they were in preschool, and adults who care for infants also should also get the vaccine. For more specific up-to-date recommendations: www.vaccineinformation.org/pertuss/.
As we enter the season for catching snowflakes and coughs, we hope none of your children catch whooping cough.
Julie Kardos, MD with Naline Lai, MD
©2011 Two Peds in a Pod®
revised Nov 16, 2011 to reflect the indications for antibiotic prophylaxis
Dr. Lai and her husband had a running debate about when to replace kitchen sponges. Today we thank guest blogger Dr. Karina Martino, Food Safety Engineer, for exposing the germs in our kitchens. We certainly learned a lot, and Dr. Lai’s husband lost a bet.
Naline Lai, MD and Julie Kardos, MD
 WHO’S THE WORST OFFENDER IN THE KITCHEN???
WHO’S THE WORST OFFENDER IN THE KITCHEN???
The winner is…….the kitchen sponge (and dishcloth)! The next worst offender is your kitchen sink. This is where vegetarians have a definite advantage since they don’t bring raw meat into their homes. There’s less chance of E. coli and Salmonella spreading, but vegetarians still have to be on the lookout for viruses and parasites.
What are the kitchen’s hot germ zones?
In descending order by highest bacterial count, these are:
1. Sponges and dishcloths
2. Sink drain area
3. Faucet handles
4. Cutting boards
5. Refrigerator handles
Here are simple steps that you can follow to create a healthier kitchen environment:
Dip sponges after every use in dilute sanitizer water (1 teaspoon bleach per quart of water); boil them for 3 minutes on a weekly basis.
• Change dish cloths daily, especially after wiping up raw meat juices.
• Wash sinks with hot soapy water prior to food preparation and before washing dishes.
• Wipe down refrigerator handles daily with dilute sanitizer water.
• Choose non-porous cutting boards that are easy to clean.
• Avoid rinsing raw meats. It contaminates the sink. If you cook meat at the correct temperature for enough time, bacteria on raw meat will be killed.
When we are handling food products everything in the kitchen must be clean, especially ourselves. It is vital to wash our hands with soap and hot water for at least 20 seconds before handling any food product. Each time you re-enter the kitchen from outdoors or any other place in the house where you might have contaminated your hands, you should wash your hands again.
Clean clothing, including aprons, is also an important part of personal hygiene. Dirty clothes and dish towels are a good place for bacteria to hide and grow. Sneezing and coughing spreads germs from our lungs, throats, and noses. When handling food, we must control the spread of germs from these natural occurrences by covering our mouths with disposable tissues and then rewashing our hands.
While the Centers for Disease Control (CDC) provides information about illness from food in homes, it does not yet offer statistics about how many people become ill from their kitchen sponges. However, here are some facts for you to keep in mind:
• The kitchen environment can be more heavily contaminated with fecal bacteria (those bacterial species associated with feces) than the bathroom, suggesting that the risk of spreading infection in the home may be highest in the kitchen-the area in the home where food is prepared.
• Microbiological surveys of domestic kitchens have found significant contamination from a variety of bacterial contaminants, including E. coli, Campylobacter, and Salmonella.
• Pathogenic organisms (germs that cause disease) have been shown to be introduced in the home by people, food, water, pets and insects.
• The domestic kitchen is not used only for food preparation, but may serve as a laundry, a workroom, and a living area for family pets. Each of these functions can serve to introduce bacterial contamination into the kitchen environment.
Moreover, research focusing specifically on the kitchen environment has found:
• 67% of kitchen sponges may be contaminated with fecal bacteria
• Contaminated cloth towels serve to transfer bacteria to dishes during drying
• 82% of sink faucet handles are contaminated during food preparation
• 60% of people do not wash the cutting board after cutting raw meat or poultry and before cutting fresh vegetables for salads
• 9% do not wash the work surface at all after cutting raw chicken
So, please don’t duplicate these mistakes! The next time that you get ready to do your dishes with your six-month-old sponge… think again!… either toss it or get your Clorox immediately!
Karina G. Martino, PhD
Dr. Martino received her Masters degree and her PhD in Food Safety Engineering from Michigan State University. A former professor at University of Georgia, she now has her own consulting business (www.kgminnovations.com) and is the mom of two children.
©2011 Two Peds in a Pod®
 If you live on the East Coast of the United States, you were bombarded today by a surprise pre-Halloween snowstorm. Now that we have our power back, we thought we’d share with you a few posts we were reminded of today:
If you live on the East Coast of the United States, you were bombarded today by a surprise pre-Halloween snowstorm. Now that we have our power back, we thought we’d share with you a few posts we were reminded of today:
©2011 Two Peds in a Pod®
Marijuana: In 2010, one out of five high school seniors and eight percent of eight graders reported using marjuana. Unlike popular belief, marijuana is addictive. Use starting in adolescence is associated with an almost 20 percent risk of dependence. It’s strong stuff. As little as five uses of pot can lead to addiction and withdrawal symptoms are similar to withdrawal symptoms from heroin. The good news is that a teen can withdraw safely at home. If your kid tells you he is not addicted and can quit at any time, challenge him to stop smoking for two weeks. If he can’t, then he is in deeper than he realizes. Pot clouds up the brain and makes it more difficult to remember recent events. Although kids say they can drive after smoking weed, their reaction time is impaired, just as it is with alcohol use. In the past researchers thought brains did not develop much in adolescence. However, brain development does continue to the early twenties, and pot can affect that development by altering mood and executive function (planning) centers in the brain. In short, marijuana causes brain damage. Steroids: It’s just as likely to be the kid who wants to look “buff,” and not just the athlete who wants to play better, who uses anabolic steroids. Addiction does occur… and in a lot of users. One-third of all users end up addicted. Not only do steroids affect muscles, but also they affect the brain. Adolescents are already known for emotional volatility and steroids heighten aggressiveness. Additionally, sex organs pay a price for steroid. In males, testicles can atrophy and breast development can occur. For females, non-reversible facial hair growth and deepening of voice are side effects. Prescription medications: Throw away those unused prescription pain killers and lock up controlled substances still in use. Prescription medications seem unintimidating to kids because they are prescribed legally and they see their parents taking them. Over the last few years, reported use of Vicodin in the past year by 12th graders ranged from about eight to ten percent. Deaths occur from overdose or from accidents from impaired driving. Data show teens listen to advice they hear from their parents and their pediatricians, even if they sometimes take time to digest and act on that advice. We pledge to do our part when we talk to your kids about the harmful effects of drug use. We urge you to continue communicating with your children, even if they are away at college. One helpful website to assist you in talking to your kids about drugs is The National Institute on Drug Abuse: http://www.nida.nih.gov/nidahome.html. Naline Lai, MD and Julie Kardos, MD ©2011 Two Peds in a Pod®
 We’re back from the national American Academy of Pediatrics conference in Boston and we’re galvanized to make a positive impact on youth. Just in time for Red Ribbon Week, the national campaign for halting substance abuse Oct 23-31 (www.redribboncoalition.com), we bring you facts for you to use as you talk about three drugs kids generally consider “harmless”: marijuana, anabolic steroids, and prescription medications.
We’re back from the national American Academy of Pediatrics conference in Boston and we’re galvanized to make a positive impact on youth. Just in time for Red Ribbon Week, the national campaign for halting substance abuse Oct 23-31 (www.redribboncoalition.com), we bring you facts for you to use as you talk about three drugs kids generally consider “harmless”: marijuana, anabolic steroids, and prescription medications.
Culled from talks given at the American Academy of Pediatrics National Convention and Exibition, 2011, by Patricia Kokotailo, MD, MPH and Greg Landry, MD, FAAP University of Wisconsin School of Medicine and Public Health, Madison, WI, John Kulig MD, MPH,FAAP, Tufts University School of Medicine, Boston. If you live in the Central Bucks area of Pennsylvania contact CBCares for more information on local Red Ribbon Week events.

Yes, yes, yes.
There are many deadly diseases we can’t prevent, but we do have the power to prevent a few. We now have the ability to prevent your children from getting some types of bacterial meningitis, pneumonia, and overwhelming blood infections. With vaccines we can prevent cases of mental retardation, paralysis, blindness, deafness, and brain infections. Immunizations are a safe way of boosting children’s natural immune systems. Yet some of our parents continue to doubt the benefits of vaccines and to fear harm from them.
Let’s look at another kind of prevention. You would never drive your car without putting a seat belt on your child. Even if you don’t know anyone who was in a fatal car accident, you still buckle you and your child up. You may know a kid who emerged from a car accident with only a scrape, yet you still buckle you and your child up.
You may never know a child who is paralyzed by polio or who died of whooping cough, but it does happen and can be prevented. Just like with car accidents, it’s better to prevent the injury than to play catch-up later. Dr. Kardos’s grandfather routinely rode in the front seat of his car without his seat belt because he “had a feeling” the seat belt might trap him in the car during an accident. Never mind that epidemiologists and emergency room doctors have shown people are much more likely to die in a car accident if they are not wearing a seat belts, he just “had a feeling.”
When it comes to your children, parental instinct is a powerful force. We routinely invite our patients’ parents to call us about their children if their instincts tell them something might be wrong, and we always welcome and at times rely on parents’ impressions of their children’s illnesses to help us make a diagnosis and formulate a treatment plan.
However, in the face of overwhelming evidence of safety and benefits of vaccines, we pediatricians despair when we see parents playing Russian roulette with their babies by not vaccinating or by delaying vaccinations. We hope fervently that these unprotected children do not contract a preventable debilitating or fatal disease that we all could have prevented through immunizations.
There is no conspiracy here. We both vaccinate our own children. We would never recommend any intervention where the potential for harm outweighs the potential for good. We have valid scientific data that every year vaccines save thousands of lives. One of them could be your child’s life.
Should you vaccinate your child?
YES!
Julie Kardos, MD and Naline Lai, MD
©2011 Two Peds in a Pod®
Visit these posts for more information about vaccines: How Vaccines Work, Evaluating Vaccine Sites on the Internet, and Closure: there is no link between the MMR vaccine and autism
Also, please visit the recent Institute of Medicine’s analysis of vaccine side effects.
Ever wonder what the school nurse or your kid’s pediatrician is looking for during a scoliosis screen? Here, in three steps, you can also monitor your child. If you are concerned, see your child’s doctor.
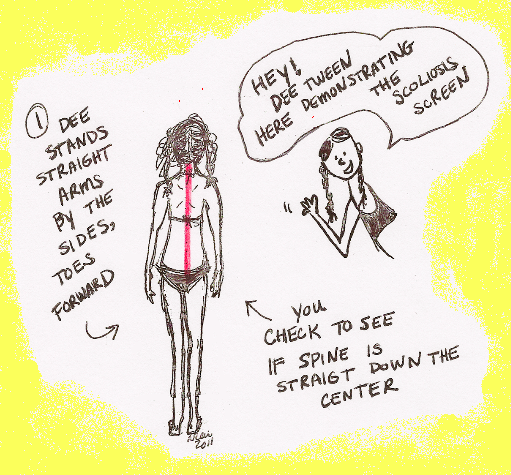
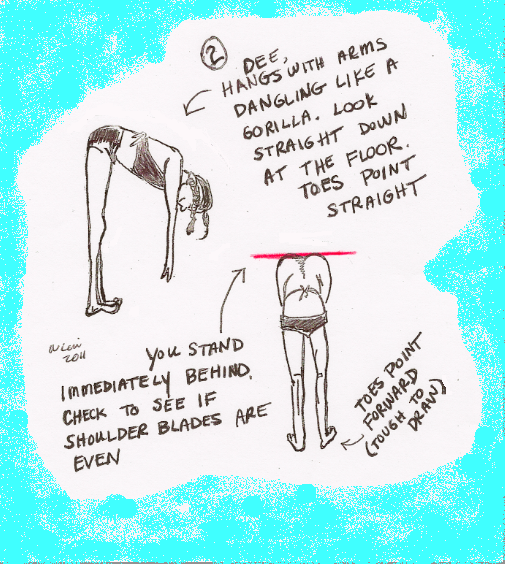
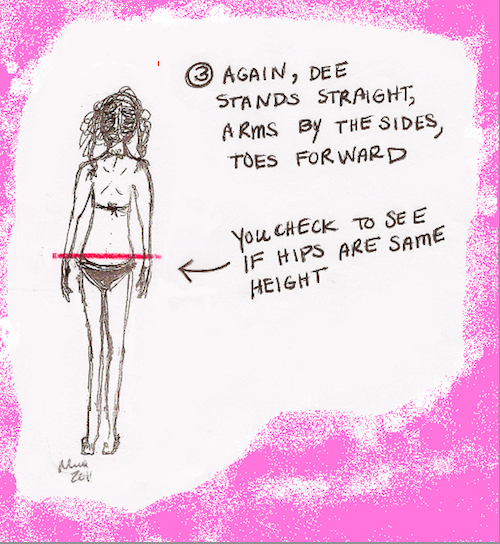
And dat is how to check dee spine!
Naline Lai, MD and Julie Kardos, MD
©2011 Two Peds in a Pod®
Although pediatricians check children’s spines for scoliosis throughout childhood, school based screens occur during pre-teen and teenage years. This timing is appropriate for school screens because most cases of idiopathic scoliosis, scoliosis with no known cause, occur during the rapid growth spurt of puberty. Eight times more common in girls than boys, scoliosis is painless and often detectable only to health care providers; minor curves are neither obvious nor disfiguring. Caught early, scoliosis can be ameliorated or corrected before adulthood when it can lead to back pain, difficulty breathing and disfigurement. Unlike what some parents think, scoliosis does not cause “bad posture.” Likewise, “bad posture” does not cause scoliosis. So, while it may cause an awkward middle school moment, scoliosis screening can actually have far reaching consequences for the future. Next up: stay tuned for a “do-it-yourself “scoliosis screen. ©2011 Two Peds in a Pod®
 I remember during my middle school days in New Jersey lining up once a year at the school nurse’s office, feeling awkward and nervous. Not only was the nurse checking our height and weight as she did every year in grade school, but now she was going to check our backs for some mysterious entity called “scoliosis.” Where I live now in Pennsylvania, many school nurses also screen students for scoliosis, a curve in the spine.
I remember during my middle school days in New Jersey lining up once a year at the school nurse’s office, feeling awkward and nervous. Not only was the nurse checking our height and weight as she did every year in grade school, but now she was going to check our backs for some mysterious entity called “scoliosis.” Where I live now in Pennsylvania, many school nurses also screen students for scoliosis, a curve in the spine.
 Depending on the degree of the curve, a child with idiopathic scoliosis might be re-examined every 4-6 months, might get an x-ray of her spine, or her health care provider might refer her to an orthopedic doctor, a specialist who cares for kids with scoliosis. Kids whose spinal curves are severe or are likely to get worse may need bracing until they stop growing. At that point the chances of the curve continuing to increase is low. Wearing a brace does not correct the curve; rather, it prevents any further curvature. Scoliosis braces are much more inconspicuous now than in the past, and can be hidden easily under clothing. Some children require surgery to correct a severe curve.
Depending on the degree of the curve, a child with idiopathic scoliosis might be re-examined every 4-6 months, might get an x-ray of her spine, or her health care provider might refer her to an orthopedic doctor, a specialist who cares for kids with scoliosis. Kids whose spinal curves are severe or are likely to get worse may need bracing until they stop growing. At that point the chances of the curve continuing to increase is low. Wearing a brace does not correct the curve; rather, it prevents any further curvature. Scoliosis braces are much more inconspicuous now than in the past, and can be hidden easily under clothing. Some children require surgery to correct a severe curve.
Julie Kardos, MD and Naline Lai, MD
While many good books have been written on the subject of how to get your kids to listen to you, today we boil this topic down to a few key sticky points. The goal is to make sure your child hears, “Please clean your room,” as well as,“Let’s go get ice cream.” Here are ways to make requests which yield results: A special note about bribes and threats: By three years old, most kids understand bribes and threats. Sounds terrible, doesn’t it? However, both can be useful when used sparingly. For example, you could offer to take your child out for ice cream, or a bike ride, or a special event, in exchange for cleaning his particularly horrendously messy room. But bribes used too often create a kid who expects to get “paid” for performing reasonable and customary personal and household tasks. Likewise, threatening a negative consequence must also be used sparingly or else you will end up with a resentful child who will have even more motivation to not listen to you. Remember to take away “extras” rather than essentials. For example, failing to listen may result in losing a finite amount of TV/videogame time. Do NOT threaten to take away eating dinner, reading with your child before bedtime or going to her best friend’s birthday party. Remember to follow through on the consequence immediately. Giving empty threats or putting off threats put you into the “nag” category. Most importantly, during any ice cream outing, bike ride, or special trip to the park, regardless if it was a planned event or a bribe, flip the table and take the time to listen to what your child has to say. Julie Kardos, MD and Naline Lai, MD Special thanks for input from Kim Ross. A first grade teacher for the past 19 years, Mrs. Ross holds a Bachlor’s degree in Early Childhood Elementary education and a Masters degree in Educational Psychology, both from Temple University. Mom of two, she also is a Certified Parenting Educator. ©2011 Two Peds in a Pod®
